
Cancer's Magic Bullet: Antibody Drug Conjugates

An exciting frontier in cancer treatment over 100 years in the making.
Shortly after her 49th birthday, Alice was diagnosed with uveal melanoma.
Uveal melanoma is a cancer that develops in the middle layer of the eye. In Alice’s case, a small (1 millimeter) tumor had formed in her eye and cells from that tumor had entered her bloodstream. By the time she was diagnosed, scans showed the melanoma cells had reached her spine and her liver.
Alice’s cancer was metastatic and she faced an uphill battle. Uveal melanoma is incredibly difficult to treat. Surgery is not an option once it has spread and standard chemotherapy offers limited benefit. Like many cancer patients, she had few effective options.
Her doctor started her on a combination of immunotherapies, but after the second dose, the side effects were too much to tolerate and she had to stop. They then tried another combination of drugs, but the tumors continued to grow. They switched to another immunotherapy, but this too, was hard to tolerate and the tumors on her spine and in her liver continued to grow.
In a moment that too many cancer patients can relate to, Alice’s oncologist shared the difficult news: There were no more standard treatments available.
However, this is not the end of Alice’s story.
To understand what happened next, we must go back a bit in time. First to the distant past and then to more recent scientific exploration.

The Concept of a Magic Bullet
In 1908, the Nobel Prize in Medicine was awarded to German physician and scientist Paul Ehrlich for his work in the field of immunology.
This age, around the turn of the century, is commonly referred to as the birth of modern medicine. Scientists were discovering the complicated mechanisms at work in our bodies. Antiseptics, vaccines, antibiotics, and diagnostic technologies were born during this era. Doctors were given tools to prevent, diagnose, and treat diseases more effectively.
In his search to understand and treat disease, Ehrlich coined the term magic bullet (based on an old German myth about a bullet that cannot miss its target).
He imagined magic bullet treatments that would kill causes of disease without harming the body itself. In 1908, Ehrlich’s laboratory created its first “magic bullet” of arsphenamine—the first antimicrobial drug (it was synthesized and therefore not an antibiotic). It was the first effective treatment for syphilis.
This treatment, considered by many to be the first chemotherapy (at least in concept), did offer a cure, but the magic was limited as it caused harsh side effects.
We have been hunting for magic bullets ever since.
The Anti-Bullet: Chemotherapy
Since its first use during World War II, chemotherapy has remained the most common cancer treatment. Chemotherapy is not a bullet. It is a sledgehammer, attacking both cancerous and healthy cells.
Most chemotherapy travels through the bloodstream entering cells indiscriminately and attacking vulnerable ones. Cells are mostly protected, except when they are dividing. Cancer cells divide often because of their characteristic rapid growth, which is why chemotherapy is effective at killing cancer cells.
Unfortunately, other healthy cells in our body are regularly dividing as well. Most often, our blood stem cells (special cells in your bone marrow that make blood), the cells that line our digestive tract, and hair follicles. This is the reason for common side effects of hair loss, nausea, and having a reduced number of white blood cells (this is called neutropenia and is important as the immune system needs white blood cells to fight off infection). Chemotherapy is a brutal treatment, causing stress and damage to the patient’s body.
However, for some, chemotherapy works. It kills cancer cells. And if the patient can tolerate the side effects long enough, the chemotherapy can provide significant benefits to shrink or at least hold off tumor growth for some time. However, most times, the treatment needs to be stopped because side-effects become too harsh or the tumor becomes resistant to the chemotherapy. There are various theories on why this happens; it is usually attributed to an additional cancer cell mutation arising. It nearly always means the patient needs a new treatment option.
It is easy to see why the magic bullet is so appealing. We have drugs that work to attack cancer, but no way to control how they are delivered once they are in the patient’s body.
The Idea Becomes a Reality
The 1970s brought about the rise of molecular biology and gene cloning. The 1980s brought about the genomics revolution. The 1990s brought about greater adoption of computers and the Internet. This has all led us to the turn of another century and another scientific age: the birth of personalized medicine, driven by advances in computation, engineering, and our understanding of complex processes within the human body. This has allowed new concepts to reach the clinic at an accelerating pace.
We’ve learned that most cells in our body express proteins on their surface as a way to communicate with other cells and interact with their environment. Cancer cells often overexpress unique proteins that aren’t used much by normal cells. These proteins vary widely by the type of cancer and the tumor’s composition, but certain types of cells and certain types of cancer consistently present the same surface proteins.
We’ve also learned that our immune systems create antibodies—specialized proteins that can recognize and help kill foreign invaders like bacteria or viruses. These antibodies have a shape that is designed to bind (like a key in a lock) to specific proteins on the surface of the bacteria or virus. Once an antibody binds to its target, it can either directly neutralize the invader, mark it for destruction by other immune cells, or block its ability to infect healthy cells. This targeted recognition and binding help the immune system effectively identify and eliminate the threat.
What a system. Once we understood this, minds got to work. In the 1970s, scientists discovered they could also create these antibodies in the lab and mass-produce them by cloning (replicating) a single antibody. This is why they are referred to as monoclonal (meaning cloned from one cell) antibodies. As technology has advanced, scientists have developed methods of creating antibodies to nearly any protein, including the unique cell-surface proteins on cancer cells.
If we could identify appropriate targets (proteins common on the surface of cancer cells, but not other healthy cells), we could design an antibody as the key to unlock it. The antibody would stick to the tumor cell and maybe even enter the cell. With the immune system, if the antibody key fits the protein lock, it gets in.
The concept of the magic bullet now appears to have its fundamental building blocks. We have chemotherapy, effective at killing cancer cells. And now we have monoclonal antibodies, a way to target specific types of cancer cells.
The magic bullet was ready to become reality, however, the road ahead was uncertain. Scientists still had to figure out how to put these building blocks together to make it all work. This process took time and effort.
Know Your ADCs
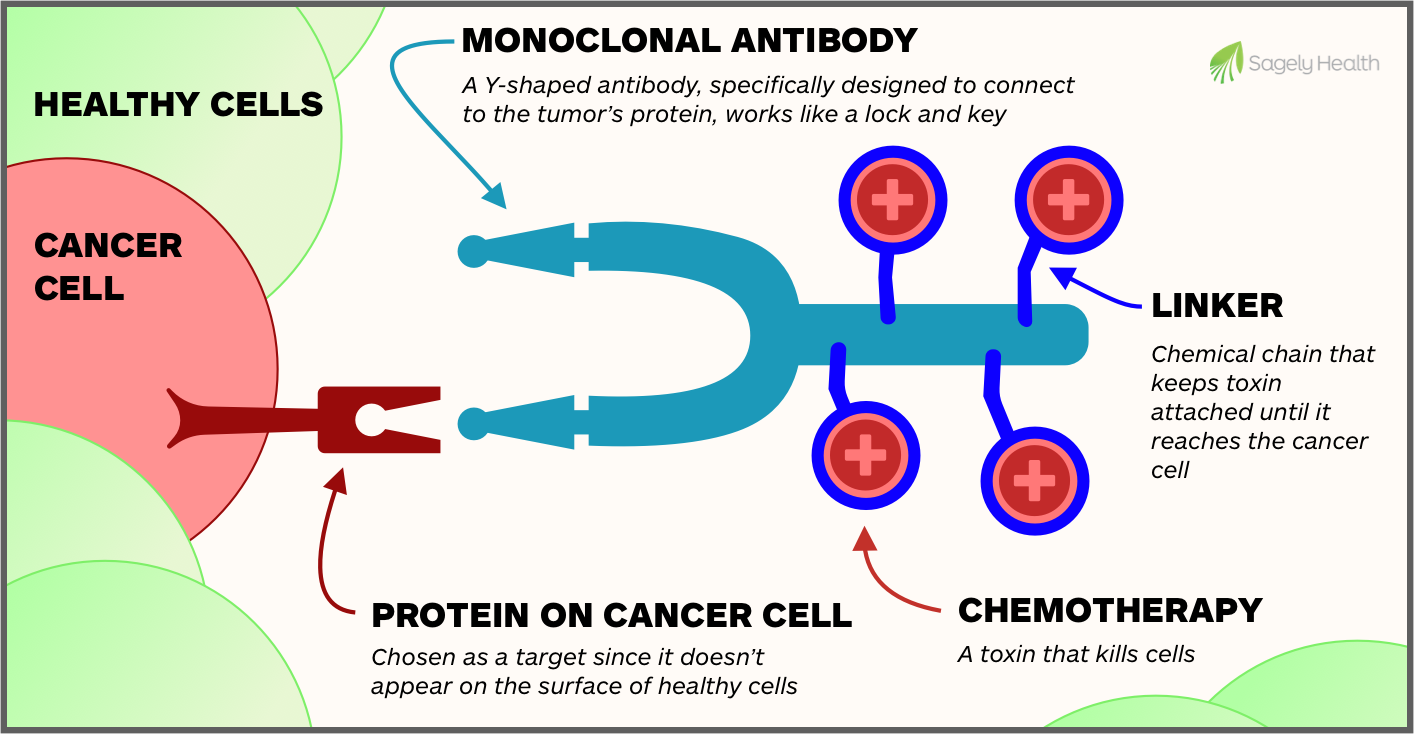
In order to know how scientists put Antibody Drug Conjugates (ADCs) together, we need to know the parts of one. An ADC is composed of three key parts (components):
- Monoclonal Antibody — Antibodies recognize and bind to proteins on the surface of cells–they connect like a lock and key. The antibody is designed to target proteins that are typically overexpressed on cancer cells. Different ADCs can use different antibodies.
- Chemotherapy (also called a toxin) — Attached to the antibody is a powerful chemotherapy drug that is released from the antibody once the antibody reaches the cancer cell. The type of chemotherapy used varies between different ADCs.
- Chemical Linker — The linker is a small chemical bond between the antibody and chemotherapy, that acts like a string. The string is designed to break and release the toxin when the antibody reaches the cancer cell.
Like most diagrams, this makes things seem simple and neat. However, the creation of effective ADCs has been a long journey and a bumpy road. Dr. Sager has described creating an ADC as “tying a boat and a plane together and expecting them to both travel smoothly.”

The Challenges
To produce an ADC, researchers have faced 4 specific challenges:
- Target Selection — Finding the best protein to target—one that would allow ADCs to attack cancer cells without harming healthy tissue was difficult. The protein should be highly present on cancer cells but minimally expressed on healthy cells. Additionally, the target should allow the antibody to cleanly bind to the cell to deliver the drug effectively. Advances in genomics, proteomics, and immunohistochemistry have helped researchers identify proteins that are uniquely or highly expressed on tumor cells.
- Antibody Development — Creating the antibody is crucial. It must be pure, stable in the bloodstream and be highly likely to bind to its target. The body must accept it and it should not produce unwanted immune system responses. Our ability to create antibodies has improved dramatically over time through various technologies and techniques such as recombinant DNA and “humanization” of non-human antibodies made in the lab.
- Linker Stability — Something has to hold the chemotherapy in place until the exact right moment. Early ADCs had issues with weak chemical linkers between the antibody and chemotherapy, which resulted in chemotherapy being released before reaching cancer cells. This could damage healthy tissue and cause harmful side effects. Advanced chemistry has allowed us to create linkers that have various releasing mechanisms. Some don’t release until they are inside the cell, some release when the antibody is broken down in the cell, and, as we’ll see with Enhertu, some are able to release their toxin at the moment the antibody binds.
- Drug Selection and Potency — It was difficult to find the right chemotherapeutic drugs that could kill cancer cells at low doses (since ADCs can only deliver a small amount to each cell). Researchers have developed highly potent cytotoxins that can kill cancer cells with just a few molecules per cell. This still leaves the question of the drug-to-antibody ratio (DAR) that should be used. This becomes a major factor in the success for Enhertu.

The First Trial, First Approval, and Beyond
In 1983, the first patients were treated with an ADC in a clinical trial. As their target, the researchers selected carcinoembryonic antigen (CEA) as it was a highly expressed protein across a variety of cancer types. Their ADC carried the chemotherapy vindesine, but also a radioactive isotope, so they could track where it went in the body.
Out of 8 patients, 4 had confirmed “localization,” meaning the antibody bound successfully to cancer cells and delivered the chemotherapy.
The researchers believed that the other patients—for whom the magic bullet did not work—may have not been expressing CEA.
However, they also found a problem while producing the ADCs, as the antibody, linker, and chemotherapy would cluster together (called aggregation) and reduce the efficacy. The boat and the plane were colliding so to speak.
Aggregation was a major problem in the early days of ADC development and was typically attributed to the ratio of antibodies to chemotherapies attached. If this ratio was off, the structure of the ADC became ineffective. It took years before these manufacturing and production issues were fixed.
As is the case with nearly all progress in cancer treatment, dedicated doctors, scientists, and patients forged ahead imagining change was possible.
Seventeen years after the first clinical trial, the FDA approved the first ADC drug, Mylotarg, in 2000. It was approved for adults with acute myeloid leukemia (AML).
Over the 2 decades that followed, 13 more ADCs were approved for cancer, including the blockbuster drug Enhertu.
Today, there are over 100 ADCs available to patients in clinical trials, spanning dozens of cancer types.

An ADC for Alice
To return to where we began. It is 2024, and Alice still does not have any remaining standard treatment options. The tumors from her uveal melanoma are growing.
It’s not clear what she should do. Fortunately for her, twelve years earlier, researchers discovered something very important about uveal melanoma.
Healthy cells in the eye, from which uveal melanoma originates, are called melanocytes. One of their jobs is to produce the protein PMEL17 to create the pigment (color) needed for the eye to function.
The researchers noticed that once a healthy melanocyte became a uveal melanoma (cancer cell), it continued to express this PMEL17 protein, even if it traveled in the bloodstream to other parts of the body. This meant that distant tumors—like the ones on Alice’s spine and in her liver—were expressing this protein.
Researchers speculated that PMEL17 would be an ideal target for an ADC. They would be able to target these cancerous melanoma cells wherever they were in the body and no other cells in the body were known to produce this protein.
In 2022, a clinical trial testing DYP688, an ADC targeting PMEL17 for melanoma patients began. It continues to recruit today. We helped Alice enroll in this clinical trial.
Since beginning treatment, which she has tolerated well, Alice’s liver metastases have shrunk by 10%. Today, her disease remains stable. This type of tumor shrinkage and stability is extremely rare in metastatic uveal melanoma cases.
Alice’s story and the story of ADCs showcase the power of resilience and the hope that comes from the pursuit of innovation. These potent and precise treatments offer new possibilities for patients who may have run out of standard options and are fighting some of the most challenging cancers to treat.
ADCs represent a promising step forward in cancer therapy, merging the precision of targeted therapy with the strength of chemotherapy in a way that aims to reduce side effects and improve outcomes for patients. As research progresses, ADCs offer hope for more effective and personalized cancer treatments.
How New Treatments like ADCs are Approved
The Food and Drug Administration approves new cancer treatments when they are shown in clinical trials to be more effective than the current approved cancer treatment for a given cancer type. The approval comes when the treatment extends lifespan without overly increasing the risks of serious side effects.
Sometimes, the incremental improvements over the existing standard of care can seem unremarkable–a small increase in response percentage for a subset of patients of a certain cancer type and treatment history, or a modest average gain of months of stable disease before the tumor grows again.
When removed from the averages and measured in months to years of a person’s life–life spent with family, life spent seeing the pace of scientific progress continue to quicken–all progress is welcome.
With some drug approvals, the approval is not so much of a testament to the new treatment’s efficacy, but the dismal state of existing treatment options.

HER2 Positive Breast Cancer
There is a protein called HER2 that is overexpressed by a number of different cancer types. HER2 plays a role in regulating cell growth so when there is too much of it, tumors can grow more aggressively. HER2 is overexpressed in approximately 15-20% of breast cancers and is also found, though at varying lower frequencies, in some gastric, lung, colorectal, ovarian, urothelial, salivary gland, and endometrial cancers.
HER2 has served as a target for treatments for decades now. In 1998, trastuzumab (Herceptin) was approved for the treatment of HER2-positive metastatic breast cancer.
It is hard to overstate what a game changer Herceptin was for patients with HER2-positive breast cancer. It represented one of the first successful targeted cancer therapies, and it effectively cut recurrence risk by half in early-stage HER2-positive cancer. It also significantly prolonged survival in advanced cases.
It also set the foundation for further development of HER2-targeted treatments and made what was once one of the most difficult-to-treat breast cancer subtypes into one that is now much more manageable with long-term treatment options.
However, for some HER2-positive patients, Herceptin doesn’t work or doesn’t work for long.
In 2013, the first ADC targeting HER2 was approved. It was called Kadcyla and it used Herceptin as its monoclonal antibody and emtansine as its toxin. It was approved for metastatic breast cancer patients who had progressed after Herceptin and chemotherapy. While it had fewer side effects, it worked only modestly better than chemotherapy, but it was another option for patients who had few.
It also advanced the promise and reality of ADCs.

The Arrival of Enhertu
In late 2019, just five days before Christmas, the FDA granted accelerated approval to a new ADC called Enhertu.
Enhertu, like Kadcyla, used Herceptin as its antibody, but for its toxin, it used a topoisomerase I inhibitor, which is a type of drug that interferes with an enzyme that unwinds and untangles replicating DNA. Essentially, as the cancerous cells are trying to replicate and grow the tumor, the drug mucks up the process and results in dead cancer cells.
The accelerated approval came after a phase II clinical trial called the DESTINY-Breast01 study. In this clinical trial, Enhertu was used to treat metastatic HER2-positive breast cancer patients whose cancer had progressed after treatment with Kadcyla, their last treatment option.
The response was remarkable: 98% of the patients benefited from the treatment and 62% saw significant shrinkage in their tumors.
The accelerated approval required that another clinical trial be performed to confirm these positive findings. Subsequent trials have demonstrated that Enhertu is much more effective than Kadcyla, but with increased frequency of side effects for some.
In the DESTINY-Breast03 trial, researchers looked at patients who had tumors that could be measured. They found with Enhertu, 82.7% of patients had some form of tumor shrinkage compared with just 36.1% in patients receiving Kadcyla.
This was an enormous step forward for ADCs. Amazingly, the plane and boat were sailing smoothly together.
Enhertu was developed in a partnership between AstraZeneca, a global biopharmaceutical company with a heavy focus on oncology, and Daiichi Sankyo, a Japanese pharmaceutical company with expertise in ADCs.
Stemming from the exciting success in treating breast cancer, the drug makers invested in clinical trials using Enhertu to treat other cancer types when HER2-positive, notably gastric cancer and non-small cell lung cancer.
Since HER2 is expressed by tumors from many types of cancer, their study, the DESTINY-PanTumor02, aimed to show high response rates in endometrial, cervical, ovarian, bladder, and bile duct cancers.
It was quite successful and in April 2024, Enhertu became the first ADC that was approved for all metastatic HER2-Positive solid tumors.
Cancer type has traditionally been the sole driver of treatment options, but now cancer characteristics (what is making the tumor grow) matter, making ADCs and other targeted therapies another powerful option in the fight against cancer.
What It Means for Patients
This is very recent in terms of the progress and adoption of cancer treatments, so there are some important things for cancer patients to know.
- Not all cancer patients have been tested for HER2, and in some cases, their oncologist may not consider the test since, in the past, it has not led to additional treatment options, but now it can. Be proactive. Ask your oncologist about your HER2 status.
- HER2 results used to be considered positive or negative, which predicted if Herceptin would work, with about 20% (1 in 5) of breast cancer patients being HER2 “positive”. However, with more powerful treatments like Enhertu, these tests are now being redefined into high, low, and negative. While Herceptin will still be used for positive (high), Enhertu works also for low too, which means that now about 75% (3 of 4) of breast cancer patients have a treatment option many would not have had before.
- Therefore, patients who were previously considered HER2-negative may actually be HER2-low, and therefore a candidate for treatments like Enhertu.
What Made Enhertu Successful
Advances in cancer treatment build upon one another. While there certainly will be winners and losers when it comes to pharmaceutical companies and their investors, generally, for cancer patients, a rising tide lifts all boats.
While progress is often incremental and modest, sometimes there are leaps like Enhertu. So, what made it different?
High Drug-to-Antibody Ratio (DAR). Prior ADCs had 2-5 molecules of chemotherapy per antibody. Remember, getting this right in manufacturing was a challenge. With Enhertu, they achieved an 8-to-1 chemotherapy to antibody ratio while keeping the drug stable and able to reach its target. Essentially, a drug-coated antibody arrived ready to attack at just the right time.
The Bystander Effect. In addition to the selection of chemotherapy, Enhertu also had innovations in the chemical linker that held the chemotherapy in place. The linker they used would release the chemotherapy when the antibody connected to the surface protein. With Kadcyla, the chemotherapy is released once pulled into the cell or when the antibody breaks down so the damage to cancer cells is limited to the cell the antibody attaches to.
With Enhertu, the toxin is released in the space just outside the cell and near other tumor cells. The toxin is also particularly effective at working through cell membranes so it could attack nearby cells from the surface.
Because cancer is made up of cells that are mutating and accumulating additional genetic changes as they grow and divide, not all cells are the same within a tumor and may not be expressing the same proteins on its surface. This characteristic, called tumor heterogeneity, is important in the case of Enhertu as a patient whose cancer expresses HER2 overall will have a mix of cancer cells: some that have lots of HER2 expressed and some that have very little.
The special release mechanism means that tumor cells that do not express HER2 could still be killed just by being near a tumor cell that has HER2 on its surface. While this sounds like it could be damaging to healthy cells, the bystander effect of chemotherapy mainly impacts the tumor environment, rather than the rest of the body.
This is not to say that ADCs are without risks and side effects. Compared to other ADCs, Enhertu has a lower side effect profile, but on the DESTINY-PanTumor2 trial, 40% of patients experienced severe side effects. Common side effects reported by patients included nausea, diarrhea, fatigue, vomiting, decreased appetite, and hair loss. Most patients could tolerate the treatment, but 8.6% of patients discontinued treatment due to side effects.
While it’s hard to hear of these challenges, Enhertu, like many ADCs gaining approval, addresses an unmet need for patients with advanced disease who have no strong alternative options.
ADCs are also changing the way scientists are developing cancer treatments. The pan-tumor (meaning all tumors known to express HER2, regardless of cancer type) approval of Enhertu highlights the importance of testing cancer biomarkers.
It also marks a transition from focusing nearly completely on cancer type. Targetable characteristics of the cancer should no longer be a secondary consideration when determining the best treatment.
The Current State of ADCs
In the past 3 years, the number of ADCs approved by the FDA has tripled. Currently, 13 ADCs have been approved by the FDA, and over 100 are being tested in clinical trials.
The theory behind ADCs was always that they could reduce the side effects for patients while increasing the efficacy of treatment. In terms of efficacy, ADCs have begun to meet the expectations of researchers. They have demonstrated a stronger anti-cancer response compared to both traditional chemotherapy and targeted therapies.
A 2024 study in Italy (2024 Boticelli et al.) showed that for traditional chemotherapy, 10% of patients had tumor shrinkage. For targeted therapies, it was about 17%. An improvement for sure, but still leaves much to be desired.
The response rate for targeted therapies can vary greatly and, in some cases, can be significantly higher. For example, a PARP inhibitor showed an overall response of 77% in BRCA-deficient ovarian cancer in one study (2019, Penson et al.).
With ADCs, the percentage of patients who experience tumor shrinkage ranges from 22-60%, depending on the cancer type and protein targeted (2024 Michelon et al., 2023, Lui et al.).
However, the increase in efficacy was only half of the promise of ADCs. When it comes to safety and side effects, ADCs still have a lot of room for improvement.
According to a meta-analysis completed in 2023 that compared the safety of ADCs and non-ADC therapies (such as chemotherapies, targeted therapies, and others), ADCs and other anti-cancer treatments had very similar rates of other side effects. ADCs had less hematologic (red and white blood cell-related) side effects, but they also had worse dry mouth, peripheral neuropathy, and reversible eye-related side effects.
We hope that continued advancements improve the safety of these drugs, but we also encourage patients going through any cancer treatment to explore additional treatments to mitigate side effects as much as possible. Too many patients struggle unnecessarily because palliative and secondary care teams are not brought in to help with managing side effects.
FDA Approved ADCs
ADCs that are approved may be prescribed by any oncologist and the list of options is growing.
| ADC (Target) | Cancer Type | FDA Approval |
|---|---|---|
| Mylotarg (CD33) | Acute Myeloid Leukemia (AML) | 2000; lower dose 2017 |
| Besponsa (CD22) | B-Cell Precursor Acute Lymphoblastic Leukemia (ALL) | 2017 adult; 2024 pediatric |
| Lumoxiti (CD22) | Hairy Cell Leukemia (HCL) | 2018 (discontinued 2023) |
| Polivy (CD79b) | Diffuse Large B-Cell Lymphoma (DLBCL), High-Grade B-Cell Lymphoma | 2019 accelerated; 2023 regular |
| Zynlonta (CD19) | Large B-Cell / Diffuse Large B-Cell Lymphoma, High-Grade B-Cell Lymphoma | 2021 accelerated |
| Adcetris (CD30) | Classical Hodgkin Lymphoma, Peripheral T-Cell Lymphomas | 2011 HL; 2018 T-Cell; 2022 pediatric CHL |
| Kadcyla (HER2) | HER2-Positive Breast Cancer | 2013 metastatic; 2019 early |
| Enhertu (HER2) | HER2-Positive & HER2-Low Breast Cancer | 2019 breast; 2022 HER2-low |
| Trodelvy (TROP-2) | Triple-Negative & HR-Positive/HER2-Negative Breast Cancer | 2020 TNBC; 2023 HR-positive |
| Padcev (Nectin-4) / Trodelvy (TROP-2) | Urothelial Cancer | 2019 Padcev accelerated; 2021 regular; 2021 Trodelvy |
| Enhertu (HER2) | Advanced Gastric / Gastroesophageal Adenocarcinoma | 2021 |
| Enhertu (HER2) | HER2-Mutant Non-Small Cell Lung Cancer | 2022 |
| Tivdak (TF) | Cervical Cancer | 2021 accelerated |
| Enhertu (HER2) | All HER2-Positive Solid Tumors | 2024 |
| Elahere (FRα) | Epithelial Ovarian, Fallopian Tube, Primary Peritoneal Cancer (FRα-positive, Platinum-Resistant) | 2022 accelerated; 2024 full |
ADCs in Clinical Trials
More FDA approvals of ADCs are expected to come. In fact, there is published clinical trial data showing strong safety and efficacy data for at least 3 ADCs that are not yet approved, but are likely to gain FDA approval, all for Non-Small Cell Lung Cancer:
- Datopotamab Deruxtecan — AstraZeneca and Daiichi Sankyo have partnered on another ADC. This one, datopotamab deruxtecan, targets a protein called TROP-2. This protein is a strong target, as it is highly expressed across various solid tumors and has nearly no expression on healthy cells. Their trial shows efficacy in Non-Small Cell Lung Cancer patients.
- Patritumab Deruxtecan — Daiichi Sankyo has another partnership with Merck and another ADC that has been granted Priority Review by the FDA. Their new ADC, patritumab deruxtecan, targets HER3 protein and has been used to treat patients with EGFR-mutated Non-Small Cell Lung Cancer.
- Telisotuzumab Vedotin — AbbVie has a Phase III clinical trial for an ADC, telisotuzumab vedotin, that is targeting c-Met Non-Small Cell Lung Cancer. Some tumors may have a mutation in the MET gene and when this happens, the surface of the tumor’s cells will have an overabundance of c-Met receptors which leads to rapid growth. These receptors can be targeted by ADCs.
Patients who participate in clinical trials are getting access to treatments that cannot yet be prescribed by any oncologist. To access ADCs in clinical trials, you must be screened by the doctors running the trial to make sure you are a match.
Sagely Health is here to support you in exploring ADCs and other innovative treatment options—whether that’s by finding and connecting you to promising treatments or helping you navigate approved therapies for yourself or a loved one.
This article was originally published on the Sagely Health blog.